Michael Riediker1*, Lidia Morawska2
1Swiss Centre for Occupational and Environmental Health (SCOEH), Winterthur, Switzerland and 2International Laboratory for Air Quality and Health (ILAQH), Queensland University of Technology, Brisbane, Queensland 4001, Australia
This article was first published in AAQR. It is reprinted here under the terms of the Creative Commons Attribution License (CC BY 4.0). Two figures were added for illustration purposes.
Citation: Riediker, M. and Morawska, L. (2020). Low Exhaled Breath Droplet Formation May Explain Why Children are Poor SARS-CoV-2 Transmitters. Aerosol Air Qual. Res. https://doi.org/10.4209/aaqr.2020.06.0304
A characteristic of the novel coronavirus disease 2019 (COVID-19) is the few cases of severely affected children. They not only rarely get symptoms but also seem to be poor transmitters. We propose that this may be explained by the mechanism of breath droplet formation, which occur during the re-opening of collapsed terminal bronchioles. Children’s lungs are still developing. Compared to adults they have few alveoli and terminal bronchioles, thus less sites of aerosol formation where virus-loaded lung lining liquid can get airborne. In addition, children have a lower respiratory minute volume and tend to have a lower viral load. These points, together with the fact that asymptomatic carriers release less aerosols than symptomatic carriers support the idea that children are indeed poor transmitters of the COVID-19 virus.
The novel coronavirus disease 2019 (COVID-19) has spread rapidly around the world. It is a highly contagious and unusual disease in that a large proportion of those able to transmit the underlying virus SARS-CoV-2 have no or barely detectable symptoms but at the same time a very high viral load in throat swabs and sputum samples (Lai et al., 2020). This is remarkable because being non-symptomatic means, for a respiratory disease, the absence of coughing or sneezing, two reflexes associated with the ejection of virus-loaded droplets that are very effective ways to transmit the virus (Chen et al., 2009). It is even more puzzling that children, although they can become infected and show virus levels similar to adults (L’Huillier et al., 2020), they seem to not contribute much to the spread of the disease (Munro and Faust, 2020). This seems counter-intuitive because children are, in general, known as big spreaders of viral respiratory diseases (Longini et al., 1982).
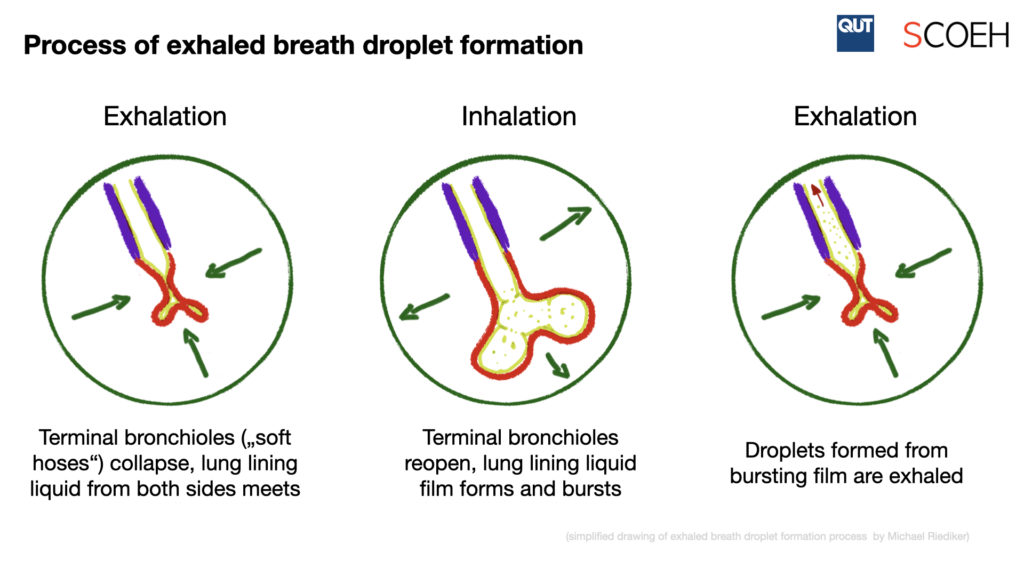
We recently proposed that the spread of COVID-19 may occur via exhaled breath droplets, also called microdroplets (Morawska and Cao, 2020; Riediker and Tsai, 2020). The mechanisms of breath droplet formation may also help explain the observed lower infectivity of children. Most of the research on exhaled breath droplet formation has so far been done in adults. Studies have shown that these droplets are formed during the re-opening of collapsed terminal bronchioles, which leads to the rupture and aerosolization of the lung lining liquid film (Johnson and Morawska, 2009; Morawska et al., 2009). A small portion of these lung lining droplets will be exhaled as aerosols and stay airborne for a prolonged time. Calculations of the number of airborne virions suggest that the concentration of exhaled breath droplets released from an asymptomatic COVID-19 positive case with high viral load can within a short time increase in a small room to the levels that can realistically cause infections (Riediker and Tsai, 2020). Exhaled droplet research has shown that speaking loudly can lead to a many-fold increase of the emitted droplet quantity, with some individuals being “super-emitters” who produce several times more droplets than a median speaker (Asadi et al., 2019). The mechanisms proposed include film rupture in the region of the vocal folds, but also higher production of droplets in the bronchioles due to more rapid inhalation and exhalation speeds compared to normal breathing. The quantity of droplets produced during breathing and speaking are below those produced during sneezing and coughing (Yang et al., 2007), but may already well explain superspreading events in choirs (Hamner et al., 2020), call centers (Shin Young Park et al., 2020) and restaurants (Lu et al., 2020) where people use loud voices.
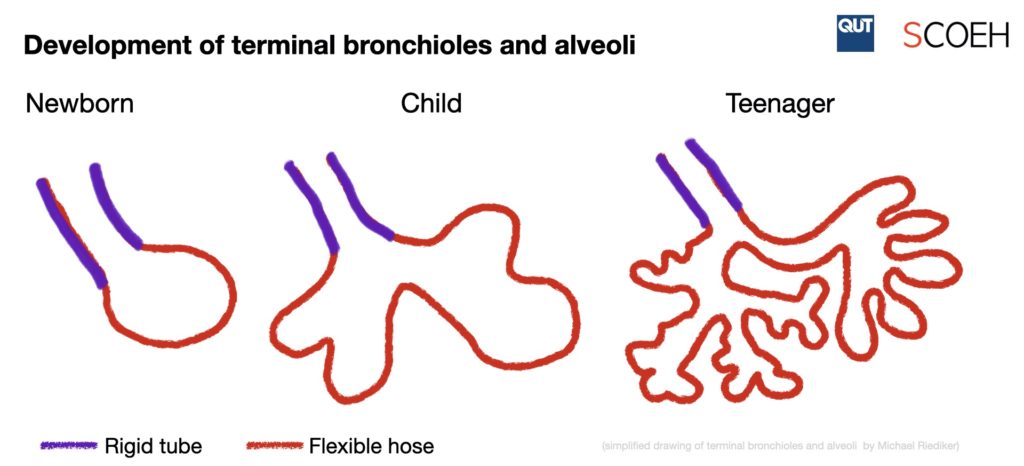
The lungs of children are not just small copies of adult lungs. After birth, the terminal bronchiole region, where most of the exhaled breath droplets seem to be formed, is not yet well developed and is still undergoing heavy transformations (Thurlbeck, 1982; Zeman and Bennett, 2006). In the post-natal phase, over 80% of the alveoli and over 25,000 bronchioles are formed during a process that goes well beyond adolescence (Dietert et al., 2000; Levitzky, 1984). This results in considerable morphological differences and associated ventilation rates per unit surface area of lower lung regions between adults and children (Ginsberg et al., 2010). More importantly, the alveolar ducts, where most exhaled breath droplets are released, are formed to a big part only during childhood (Thurlbeck, 1982). Thus, children have not only a reduced breathing volume but – much more importantly – significantly less locations where droplet formation by liquid film rupture can occur. Very little data is available on exhaled breath droplets emitted by children. Studies have shown that symptomatic children can exhale respiratory viruses but provided few details about the droplet size distribution (Gralton et al., 2013; Stelzer-Braid et al., 2009). Indirect evidence comes also from research on rhinovirus infections in asthmatic children, where the change of viral infection location from nose to lower regions of the airways could clearly be seen in the symptoms but was barely detectable in the exhaled RNA levels (Tovey et al., 2015). Clearly more research is needed to understand the exhaled breath droplet formation processes in children and how this may influence the transmission likelihood of virus-loaded droplets. Besides morphometric differences in the lower lung regions of adults and children, the role of liquid surface tension in the terminal bronchioles, including the physiological control mechanisms for mucus and surfactant formation and the response to indoor and outdoor humidity and temperature changes, should be assessed.
.